
May 24, 2023
When treated effectively, HIV/AIDS is no longer a terminal illness, but a manageable chronic condition. Despite great progress in developing effective therapies, a significant number of Americans continue to be disproportionately at high risk for infection and death. This is especially the case for certain racial and ethnic minorities, the uninsured, low-income individuals and those living far from experienced treatment centers.
Preventive Medicines for HIV/AIDS Have No Out-of-Pocket Costs, For Now
Currently, employer-sponsored group health plans must cover out-of-pocket (OOP) costs for preventive HIV medications known as pre-exposure prophylaxis (PrEP). Under the Affordable Care Act’s (ACA) preventive coverage requirement, most group health plans must cover 100% of the OOP costs for all preventive services given an “A” or “B” rating by the U.S. Preventive Services Task Force (USPSTF). The USPSTF issued an “A” rating of evidence for effectiveness of PrEP treatment for individuals at high risk of contracting HIV, requiring group health plans to begin covering 100% of the costs in 2020 (2021 for calendar year health plans). Although ongoing litigation as of December 2022 has challenged the constitutionality of the ACA’s preventive services requirement, group health plans must still cover these services, including PrEP, without cost sharing while the legal challenge is underway.
Sign up for the Business Group’s Policy & Advocacy Newsletter for more insight into this evolving regulatory and legislative landscape, along with considerations for employer-sponsored coverage of HIV/AIDS treatment and other prevention services.
Given the lack of OOP costs for employees and family members to access PrEP (see text box), disparities in utilization of preventive medicines cannot be explained by cost alone. Stigma about seeking treatment, a lack of specialized providers and transportation, particularly in Black and Hispanic/Latino communities, along with a lack of awareness about low- or no-cost treatments, has exacerbated long-standing disparities.1,2,3
Research suggests that more than 90% of new HIV infections are the result of patients not receiving proper preventive care, and many of these cases could be averted through early diagnosis and appropriate ongoing treatment.4 Employers are in an excellent position to use education campaigns, plan design incentives and other tools to help increase awareness of, and access to, preventive treatment. Given the high cost of treatment for HIV/AIDS, employers can benefit from a prevention strategy that encourages appropriate use of PrEP for individuals at high-risk for infection.
This resource discusses HIV prevention strategies along with important considerations for employers as they support employees and dependents living with HIV/AIDS.
Assessing the Disproportionate Burden of Disease
There has been much progress made to address the impact of HIV/AIDS, but health disparities persist, suggesting a need for more nuanced approaches to prevention efforts. Though the overall number of new HIV diagnoses has declined in recent years, tens of thousands of new diagnoses continue to occur in the U.S. each year, with disproportionate impacts among certain populations and regions.5
According to the Centers for Disease Control and Prevention (CDC), persisting racial and ethnic disparities in new HIV diagnoses are driven in part by underlying barriers to health care and systemic inequalities such as racism, homophobia, poverty, stigma and discrimination.3 Among new HIV diagnoses in 2020, 68% were men who have sex with men (MSM), 22% were infected by heterosexual contact and 7% through injection drug use.3 Black Americans accounted for 42% of all new HIV diagnoses in 2020, although they comprise only about 13% of the U.S. population (Figure 1).3 Similarly, despite making up only 0.5% of the U.S. adult population, transgender individuals account for 2% of diagnoses of HIV infection.6,7 These data points underscore the need for targeted treatment and prevention efforts.
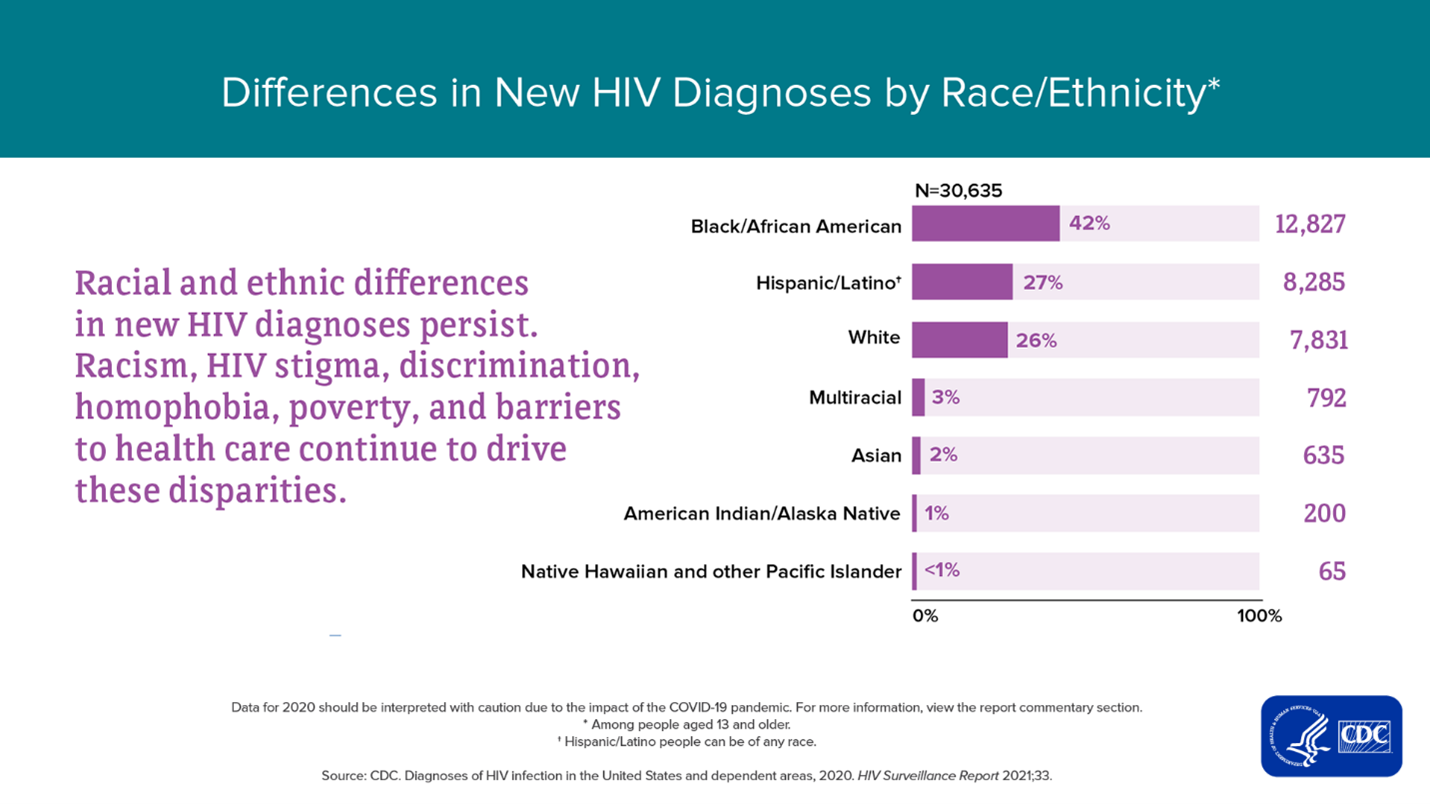
Source: From “Diagnosis of HIV infection in the United States and Dependent Areas,” 2020, HIV Surveillance Report. CDC.
Viewed geographically, the majority of individuals who receive a diagnosis tend to live in urban metropolitan areas with populations of 500,000 or more.8 The federal government has targeted its efforts on first addressing HIV in areas with the highest burden of disease, including the 48 counties, plus Washington, DC, and San Juan, and an additional seven states with a substantial number of HIV diagnoses in rural areas (Figure 2).9
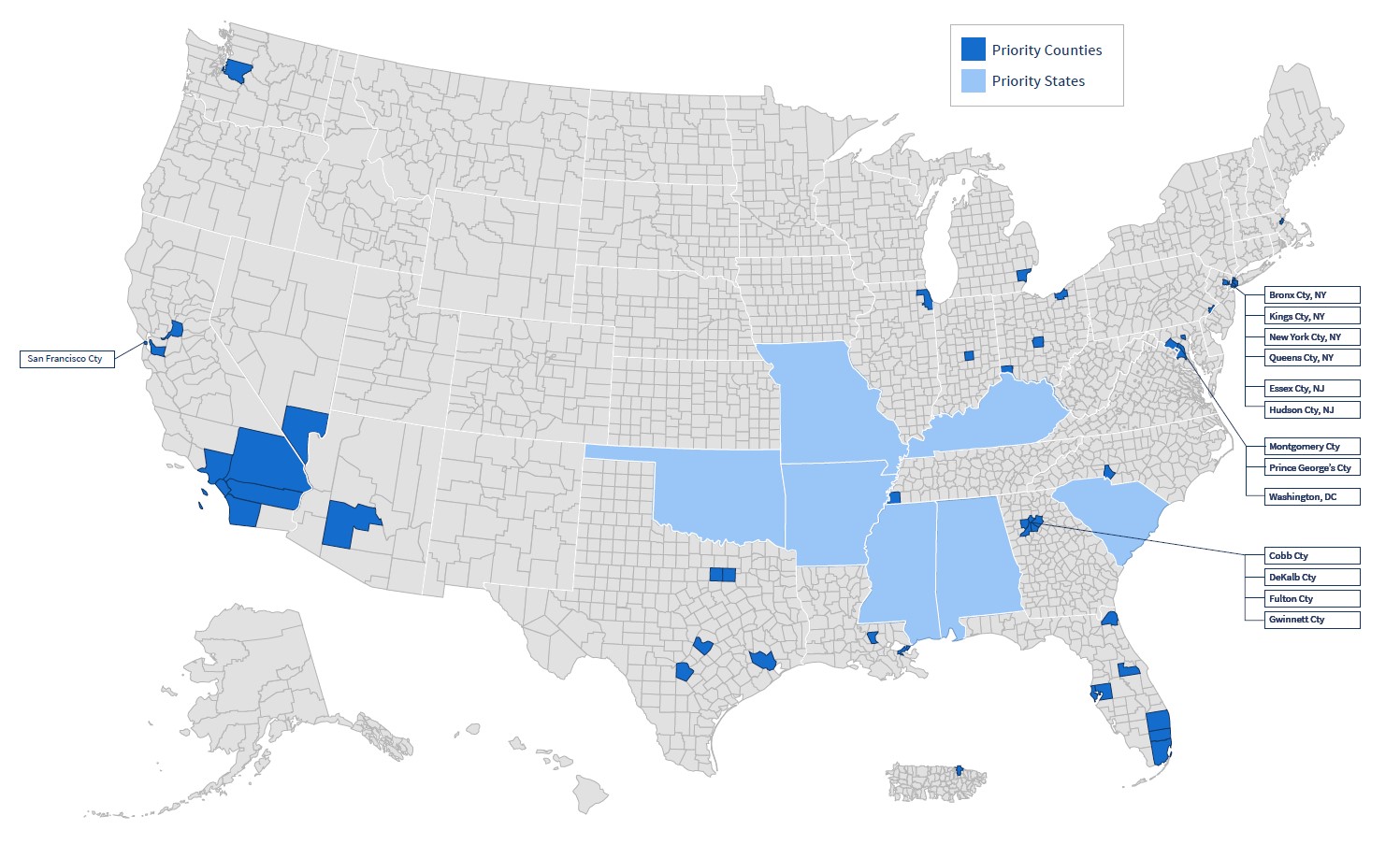
Source: From “Priority Jurisdictions: Phase 1,” 2020, Office of Infectious Disease and HIV/AIDS Policy, HHS.
Global Implications
Americans comprise only 1.2 million of the 38 million people in the world currently living with HIV.11 It is important that employers keep the global impact of this disease in mind when considering HIV prevention and treatment strategies, especially for multinational companies with global operations/workforces. Employers should be aware of global disparities related to the availability of PrEP outside the U.S., insurance exclusions for HIV care/treatment and varying levels of stigma that can create challenges for consistently addressing HIV. Business Group on Health has several global-focused insights on this issue and tips for mainstreamed HIV/AIDS coverage.
Excellent Tools Exist to Prevent HIV Infection and Progression to AIDS
Along with non-pharmaceutical prevention strategies (e.g., use of condoms, routine testing, sexual abstinence and needle exchange programs), those at risk for HIV infection may also be able to take advantage of treatments that prevent infections and the progression of HIV to AIDS, as shown in the boxes below.
Key Pharmaceutical Treatment and Prevention Options for HIV/AIDS
| Preexposure prophylaxis (PrEP): The use of antiretroviral drugs by HIV-negative individuals before potential exposure to HIV to prevent contracting HIV through sex or injection drug use. PrEP is generally taken in the form of a daily pill, though new PrEP treatments that are administered via injection less frequently are entering the market. |
| Post-exposure prophylaxis (PEP): Emergency use of antiretroviral medication for 28 days by HIV-negative individuals to prevent HIV infection within 72 hours following exposure to HIV. |
| Antiretroviral therapy (ART): Refers to the lifelong use of antiretroviral drugs by HIV-positive people to achieve viral suppression, which reduces the amount of HIV cells in the body to a level so low that it is undetectable and untransmissible to another individual. |
The Role of PrEP and PEP in Preventing New HIV Infections
Pre- and post-exposure prophylaxis medications are together key parts of an effective prevention strategy for ending the HIV epidemic.12
PrEP Effectiveness and Uptake
PrEP medications block HIV cells from replicating, which prevents transmission from an HIV-positive individual to an HIV-negative person. When an HIV-negative individual takes PrEP as prescribed, the risk of getting HIV through sex decreases by 99% and through shared needles for drug users by 74%.13 Despite excellent effectiveness and zero OOP costs for insured individuals (per its USPSTF “A” rating), PrEP is highly underutilized. Of the approximately 1.2 million high-risk individuals in the U.S. who might benefit from taking PrEP, only about 25% actually use it. Uptake for at-risk racial minorities and lower-income individuals is even lower.14
- PrEP and the high cost of not using it: Brand-name PrEP costs nearly $24,000 for a year supply, but starting in 2021, generic competition began to bring down these costs. Even with this high cost for the preventive medicine, the potential alternative is a lifetime of HIV treatment, which is estimated to cost an individual and their employer/insurer over $400,000.15,16 PrEP is not intended to be taken for the duration of a patient’s life, but rather only during the timeframe when a patient is most at risk (e.g., while in an ongoing relationship with a person living with HIV, consistently not using a condom/having multiple sexual partners in short periods of time or using/sharing drug injection equipment).17,18
Progress Update
CDC data released in May of 2023 reports a 12% drop in the estimated number of new HIV infections from 2017 to 2021, driven mainly by decreases in cases amongst young gay and bisexual men. This research suggests that the progress made in HIV prevention efforts thus far has in part been enabled through improved access to PrEP, testing and treatment services.
PEP: An Additional Level of Infection Prevention
PEP is another effective prevention tool. PEP is prescribed for emergency use only and should be taken as soon as possible within a 72-hour window after a possible HIV exposure.5 Those prescribed PEP need to take it for 28 days after exposure.19 While observational research suggests PEP is more than 80% effective in preventing HIV infection if taken as prescribed, it is not a substitute for other prevention measures (i.e., PrEP, using condoms, testing, sexual abstinence and not sharing drug injection equipment), especially among individuals with ongoing exposure risks.20,21
- PEP costs and coverage: PEP has not been rated by USPSTF, and health plans are not required to cover it or eliminate cost sharing. The OOP cost of PEP can range from $600 to $1,000 for a 28-day cycle of treatment.19
Needle Exchange Programs: Another HIV Prevention Tool
Sharing syringes is the second riskiest behavior behind receptive anal sex for getting HIV. Fortunately, however, clean needle exchange programs can prevent transmission.22 Most implementation has been at the community level, and funding generally comes from local health departments or charities. Needle exchanges are highly stigmatized by those who think they promote drug use. Employers generally do not fund or provide needle exchange services, given concerns about employees using drugs.
The Role of ART in Preventing Progression from HIV to AIDS in HIV-Positive Individuals
ART is the standard of care for people living with HIV. It is a combination of medicines taken daily, referred to as an “HIV treatment regimen.” These medications prevent the HIV virus from multiplying, reducing the amount of HIV in the body (i.e., the viral load) and giving the patient’s immune system a chance to recover and produce more infection-fighting CD4 immune cells. Even though some of the virus remains in the body, with the virus suppressed, the patient’s immune system can more effectively fight off infections and certain HIV-related cancers.23
The CDC reports that consistent treatment can significantly suppress the HIV viral load in the patient’s blood to where it is undetectable, effectively removing the risk of progression to AIDS, transmission through sex and potentially through other transmission routes like breastfeeding and needle sharing.24,25
There are several medications available to be taken as part of an effective HIV treatment regimen. They are grouped into seven different drug classes by the mode in which they fight the virus.23 Patients are usually placed on three medications from at least two different drug classes.23
ART Adherence and Uptake
People should initiate ART immediately upon receiving an HIV diagnosis and will take it for the rest of their lives to avoid progression to AIDS. Despite numerous ART drug options available in the market and clear evidence of effectiveness, many people living with HIV are not adherent to treatment. For example, one analysis looking at people diagnosed with HIV in the U.S. – 93% of whom are on ART – found that only about one-third maintained viral suppression over a 1-year period.26,27 Poor adherence to ART is associated with mental health conditions, substance use disorder, unstable housing, concern about side effects and difficulty accessing prescribing physicians.28 For those not on ART, cost is a common reason cited for not taking it.26
The U.S. has the highest ART drug prices and the lowest HIV viral suppression rate (57%) among other comparable high-income countries (for example, Switzerland and the United Kingdom have achieved HIV suppression rates of 89% and 87%, respectively).29 Effective ART regimens have made a manageable chronic condition out of a virus that was once a death sentence, but they only work if people take them. This is evident in how the COVID pandemic disrupted health services for people living with HIV—particularly among communities of color—which may lead to elevated AIDS cases down the road.30
ART: Highly Effective, Highly Priced
Whereas PrEP’s “A” rating from the USPSTF currently makes it “free” to patients, ART is generally covered, but subject to standard health plan design for specialty medicines. The average wholesale price (AWP) of ART in the U.S in 2022 is around $36,000 per year, with medication prices rising significantly in recent years.31 From 2012-2018, the AWP of ART treatment regimens increased 34%, 3.5 times faster than the rate of inflation.32 The lack of affordability remains a barrier to consistent ART uptake and adherence, particularly for individuals belonging to marginalized and at-risk communities.33,34 As treatments improve, the lifetime cost of HIV treatment increases because patients are living longer. Given the relatively small portion of the population that is HIV positive and high costs of treatment, prevention is even more important to alleviate disparities and control costs.
Evolving Treatment and Research Landscape
Research is underway to develop long-acting therapies that can be taken less frequently and serve as an alternative to daily dosing. There is optimism that such therapies could improve adherence and long-term costs, as well as reduce toxicity.35 In addition to this evolving treatment landscape, the National Institute of Allergy and Infectious Diseases (NIAID) has launched clinical trials to evaluate experimental HIV vaccines based on a messenger RNA (mRNA) platform – a technology utilized in COVID-19 vaccines.36
Employer Considerations
Employers looking to increase appropriate utilization of highly effective prevention medicines for HIV/AIDS need to keep several factors in mind. Note that all individuals being considered for PrEP must have a recently documented negative HIV test.37
The Impact of PrEP on Health Care Costs
A 2021 drug trend report by Evernorth estimates that HIV drug trend will remain at or above 6% through 2023.38 While brand-name PrEP costs about $24,000/per year on average and ART costs are rapidly rising, this is balanced by a number of generic PrEP alternatives that have reached the market in recent years.39,40 The population for whom PrEP is appropriate is relatively small, though employers in industries with higher rates of employees who are at risk for transmission (e.g., airlines, hospitality) may see a greater impact. According to the Business Group’s 2023 Large Employers’ Health Care Strategy and Plan Design Survey, when asked about the top conditions impacting their company’s health care costs and trend over the past 3 years, only 1%-2% of employers marked HIV/AIDS as a top cost driver.
To reduce unit costs of PrEP and ART, some PBMs have begun to exclude specific PrEP and ART medications from their formularies. For both PrEP and ART, there are several available medications, including generics for many name-brand drugs, so it is possible to maintain access while driving down costs through exclusions or tiering. Still, swift exceptions to these exclusions need to be processed by PBM and health plan partners when non-formulary medications are necessary. Some providers may prescribe brand-name only because of perverse incentives that garner them additional revenue for putting patients on high-cost drugs; employers should be ready to support employees who have increased friction with their providers if only generics are covered.40
Stigma and Behavioral Health-related Considerations
People living with or at-risk for HIV/AIDS infection have been stigmatized for decades. This has resulted in a lack of infrastructure to support these individuals, as well as a reticence among them to seek care. There is strong evidence that people adherent to PrEP and ART have better mental health outcomes. Not having to worry about a deadly disease because you have preventive treatment is impactful.41 Meaningful coverage of PrEP, PEP and ART gives people who could benefit from them peace of mind that they will not be infected.
Global Considerations for PrEP
The impact of and response to HIV/AIDS varies around the globe. For multinational employers, HIV/AIDS prevention requires a nuanced approach. Roughly half the people using PrEP in 2020 lived in Africa and roughly a quarter lived in the United States. Further, 130 countries have adopted PrEP guidelines, with an additional 23 countries reporting they plan to do so (Figure 3).42 As part of a global consistency strategy for inclusive benefit design, companies can coordinate with their broker and insurer partners to see if PrEP coverage is feasible. There are some markets where coverage might not be possible due to HIV/AIDS exclusions, unavailability of medications, criminalization of people with HIV or stigma surrounding HIV/AIDS significantly depressing uptake in medication usage.42,43
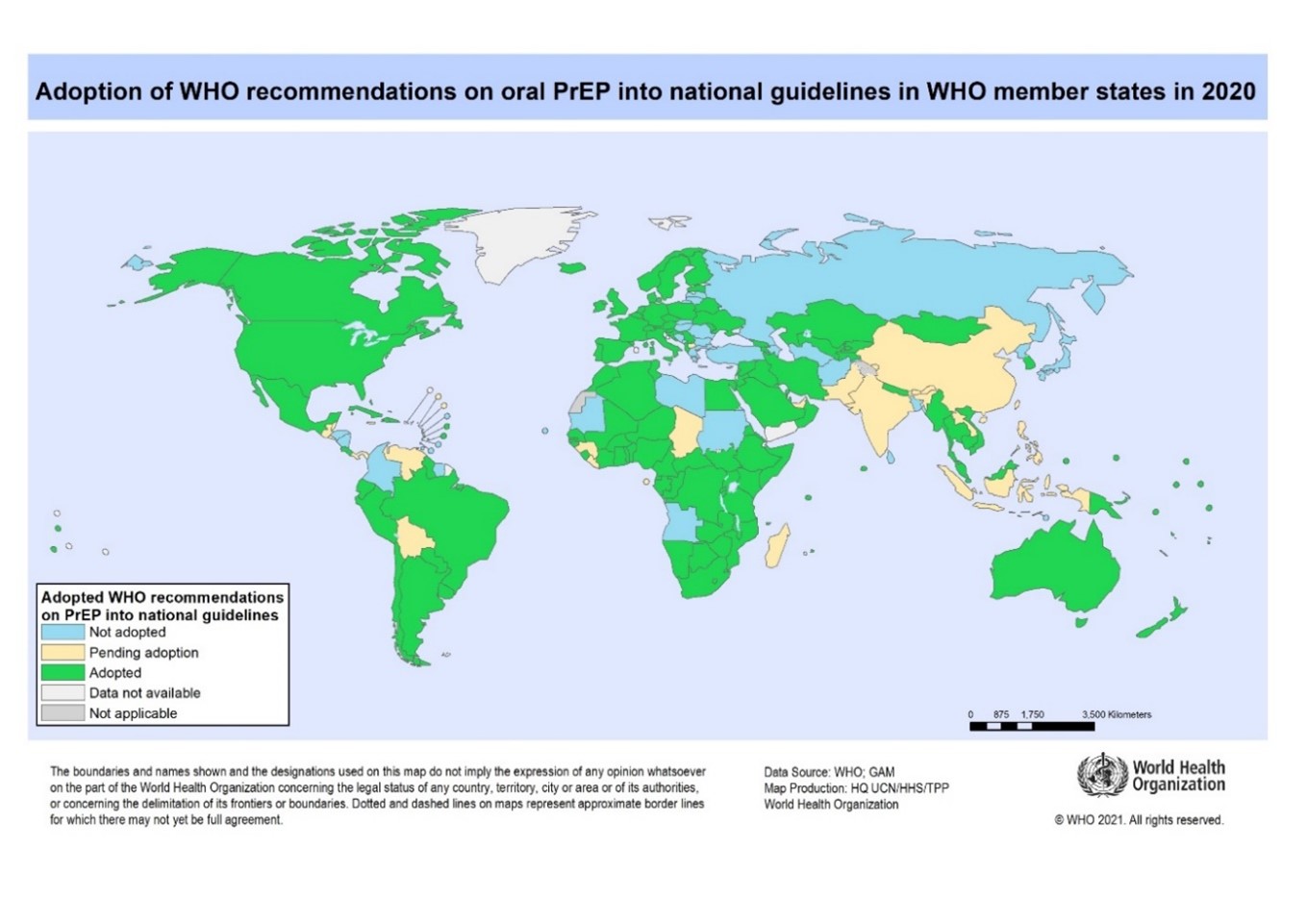
Source: From “Global State of PrEP," 2022. World Health Organization.
Legal/Regulatory Considerations
In recent years, legal challenges have emerged arguing that the ACA’s preventive service coverage requirements are unconstitutional, most recently regarding the legal authority of the USPSTF and religious exemptions for the coverage of certain required preventive services.44,45 Given the current legal and regulatory landscape, including the uncertain timing of recent constitutional challenges working their way through the judicial process, employers can evaluate their own plans to assess how they will cover and address cost sharing for PrEP if required preventive care coverage – including USPSTF-related recommendations for the medication – are deemed unconstitutional and thus no longer required under the ACA. Continuing to cover preventive services, even without a mandate, presumably could help safeguard covered employees’ ability to afford preventive services and treatment such as PrEP.
Employer Recommendations
Coverage and Benefit Strategies for Preventing HIV and AIDS
- 1 | Incorporate HIV/AIDS messaging as a part of anti-stigma campaigns, alongside other conditions you may be focused on. Partner with employer resource groups (ERGs) to craft culturally sensitive communications to and about the LGBTQ+ community in your broader messaging. ERGs can be a good place to start targeted messaging to those who would likely benefit most from a robust prevention, testing and treatment approach.
- 2 | Discuss with counsel your plan and coverage approach to understand how pending litigation and/or legislation may affect coverage requirements of preventive services such as PrEP. Subscribe to the Business Group’s Policy & Advocacy Newsletter for pertinent updates.
- 3 | Ask your health plan to assess network coverage for facilities that are culturally competent in prescribing and monitoring the use of and adherence to PrEP and ART. Consider working with third-party vendors that provide navigation services for LGBTQ+ to help them identify high-quality, affirming providers.
- 4 | Work with your PBM and health plan partners to assess potential pharmaceutical exclusions where effective drug/treatment alternatives exist for PrEP and ART. Multiple drugs are available for both of these treatments, including generics, and a targeted formulary may be able to drive down costs for your plan members and the company. Any exclusions must include expedient exceptions where necessary.
- 5 | Communicate the benefits of robust coverage and consider reducing cost sharing for HIV tests and screening services. Employers can incorporate HIV testing into on-site and mobile health offerings, which can be a good opportunity to communicate the availability of highly effective HIV/AIDS prevention tools.
- 6 | If you use a mail-only strategy for specialty medicines, consider exceptions for PrEP and ART given that plan members may desire additional privacy due to stigma associated with HIV/AIDS.
- 7 | Develop an HIV communication strategy for your entire employee population and couple it with a more targeted approach to better reach those at risk. Normalize speaking about the disease to make patients and/or those at risk feel less isolated and more supported.
- 8 | Keep in mind the role social determinants of health (SDOH) play in the health of your workforce outside the health care system. SDOH will have an impact on HIV/AIDS medication uptake and adherence rates. Address barriers to treatment outside the health care system that your plan members living with or at-risk for HIV face by consulting with ERGs to identify challenges areas, such as transportation to gender-affirming providers. Business Group on Health has curated a comprehensive SDOH guide for well-being and benefits leaders seeking to understand and address the impacts of SDOH.
- 9 | Ensure that your existing resources such as care management, navigation teams and other relevant health partners are equipped with appropriate information on best sites of care for HIV/AIDS services and can integrate behavioral health support for these patients. Newer navigator programs that cater to populations with specific challenges accessing appropriate, affirming care, such as employees and family members who are LGBTQ+, may be best able to help connect these individuals to providers with experience and empathy for their situation.
- 10 | Consider virtual care solutions that may be able to extend the availability of prescribing physicians, especially for employees in rural areas and those with high levels of stigma surrounding people who are LGBTQ+. This is not a complete solution for people in need of preventive services for HIV, because there are doctor visits and tests necessary for ongoing PrEP and ART treatment, but it can be one part of a strategy for increasing access.
- 11 | Given that PEP is used only in acute emergency situations and is a powerful HIV prevention tool, employers should make sure that PEP is covered in their medical plans. The majority of commercial insurance plans, including those offered by self-insured employers, already do so.
Global Coverage for HIV/AIDS
Global and multinational employers need to stay informed on the global state of coverage. Consider working with your broker and/or insurer partners to identify coverage gaps and assess whether coverage for HIV treatments such as PrEP is feasible. In addition, consider the regional nuances and practical implications regarding stigma associated with HIV/AIDS.
Moving Forward to Prevent Infections and Help End the HIV/AIDS Epidemic
HIV has undoubtedly made its mark across the globe, infecting more than 70 million people worldwide and claiming 35 million lives since the start of the epidemic in the 1980s.46 Despite the progress that has been made in increasing access to and coverage of preventive HIV treatment, uptake is low, and disparities in new infections persist, underscoring that there is still much more to do. Employers have several options available to them to increase access to treatment and prevention tools like PrEP, PEP and ART that are highly effective, though expensive in the short term. Nevertheless, employers are behooved to take a close look at their HIV/AIDS prevention strategy to improve health and mitigate longer-term costs.
- 1 | Bonacci RA, Smith DK, Ojikutu BO. Toward greater pre-exposure prophylaxis equity: Increasing provision and uptake for Black and Hispanic/Latino individuals in the U.S. American Journal of Preventive Medicine. 2021;61(5):S60-S72.
- 2 | Marcus JL, Killelea A, Krakower DS. Perverse incentives — HIV prevention and the 340B drug pricing program. New England Journal of Medicine. 2022;386(22):2064-2066.
- 3 | Centers for Disease and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas 2020. May 24, 2022. Available at: https://www.cdc.gov/hiv/library/reports/hiv-surveillance/vol-33/index.html. Accessed November 28, 2022.
- 4 | National Center for HIV, STD, and TB Prevention (NCHHSTP) From CDC: 9 in 10 New U.S. HIV Infections Come From People Not Receiving HIV Care. November 10, 2020. Available at: https://clinicalinfo.hiv.gov/en/news/cdc-9-10-new-us-hiv-infections-come-people-not-receiving-hiv-care. Accessed November 28, 2022.
- 5 | Centers for Disease Control and Prevention. HIV Basic Statistics. June 21, 2022. Available at: https://www.cdc.gov/hiv/basics/statistics.html. Accessed November 28, 2022.
- 6 | UCLA School of Law Williams Institute.Subpopulation: Transgender people. Available at: https://williamsinstitute.law.ucla.edu/subpopulations/transgender-people/. Accessed November 28, 2022.
- 7 | Centers for Disease Control and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas 2020: Special Focus Profiles. May 24, 2022. Available at: https://www.cdc.gov/hiv/library/reports/hiv-surveillance/vol-33/content/special-focus-profiles.html. Accessed November 17, 2022.
- 8 | Patel D, Taylor-Aidoo N, Marandet A, Heitgerd J, Maciak B. Assessing differences in CDC-funded HIV testing by urbanicity, United States, 2016. Journal of Community Health. 2019;44(1):95-102.
- 9 | Office of Infectious Disease and HIV/AIDS Policy, HHS. Overview: What Is Ending the HIV Epidemic in the U.S.? July 1, 2022. Available at: https://www.hiv.gov/federal-response/ending-the-hiv-epidemic/overview. Accessed November 28, 2022.
- 10 | Office of Infectious Disease and HIV/AIDS Policy, HHS. Priority Jurisdictions: Phase I. November 3, 2020. Available at: https://www.hiv.gov/federal-response/ending-the-hiv-epidemic/jurisdictions/phase-one. Accessed November 28, 2022.
- 11 | I.S. Department of Health and Human Services. After 40 Years of Progress, It’s Time to End the HIV Epidemic. July 7, 2021. Available at: https://www.hiv.gov/blog/after-40-years-progress-it-s-time-end-hiv-epidemic. Accessed November 28, 2022.
- 12 | HIV.gov. HIV Treatment as Prevention. June 17, 2022. Available at: https://www.hiv.gov/tasp. Accessed November 28, 2022
- 13 | Centers for Disease Control and Prevention. PrEP Effectiveness. June 6, 2022. Available at: https://www.cdc.gov/hiv/basics/prep/prep-effectiveness.html. Accessed November 28, 2022.
- 14 | Varney S. HIV preventive care is supposed to be free in the US. So, why are some patients still paying? Kaiser Family Foundation. March 3, 2022. Available at: https://khn.org/news/article/prep-hiv-prevention-costs-covered-problems-insurance/. Accessed November 28, 2022.
- 15 | Watson S. How much does Truvada for PrEP cost? WebMD. May 9, 2022. Available at: https://www.webmd.com/hiv-aids/how-much-truvada-for-prep-costs. Accessed November 28, 2022.
- 16 | Bingham A, Shrestha RK, Khurana N, Jacobson EU, Farnham PG. Estimated lifetime HIV-related medical costs in the United States. Sex Transm Dis. Apr 1 2021;48(4):299-304.
- 17 | Human Rights Campaign Foundation. Is PrEP Right For Me? February 2017. Available at: https://www.hrc.org/resources/is-prep-right-for-me. Accessed November 28, 2022.
- 18 | Juusola JL, Brandeau ML, Owens DK, Bendavid E. The cost-effectiveness of preexposure prophylaxis for HIV prevention in the United States in men who have sex with men. Ann Intern Med. Apr 17 2012;156(8):541-550.
- 19 | King County. PEP (Post-exposure prophylaxis). February 7, 2022. Available at: https://kingcounty.gov/depts/health/communicable-diseases/hiv-std/patients/post-exposure-prophylaxis.aspx. Accessed November 28, 2022.
- 20 | Arkell C. Post-exposure prophylaxis (PEP). CATIE. Available at: https://www.catie.ca/post-exposure-prophylaxis-pep. Accessed November 28, 2022.
- 21 | Centers for Disease Control and Prevention.What is PEP? July 12, 2022. Available at: https://www.cdc.gov/hiv/basics/pep/about-pep.html. Accessed November 28, 2022.
- 22 | Centers for Disease Control and Prevention. HIV and Injection Drug Use. April 21, 2021. Available at: https://www.cdc.gov/hiv/basics/hiv-transmission/injection-drug-use.html. Accessed November 28, 2022.
- 23 | National Institutes of Health Office of AIDS Research. HIV Treatment: The Basics. August 16, 2021. Available at: https://hivinfo.nih.gov/understanding-hiv/fact-sheets/hiv-treatment-basics.
- 24 | Centers for Disease Control and Prevention. HIV Treatment. July 14, 2022. Available at: https://www.cdc.gov/hiv/basics/livingwithhiv/treatment.html. Accessed November 8, 2022.
- 25 | Centers for Disease Control and Prevention. HIV Treatment as Prevention Overview. July 21, 2022. Available at: https://www.cdc.gov/hiv/risk/art/index.html. Accessed November 17, 2022.
- 26 | Centers for Disease Control and Prevention. HIV Surveillance Report. Behavioral and Clinical Characteristics of Persons with Diagnosed HIV Infection—Medical Monitoring Project, United States, 2018 Cycle (June 2018–May 2019). Available at: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-special-report-number-25.pdf. Accessed November 28, 2022.
- 27 | Centers for Disease Control and Prevention. Evidence of HIV Treatment and Viral Suppression in Preventing the Sexual Transmission of HIV. June 2, 2022. Available at: https://www.cdc.gov/hiv/risk/art/evidence-of-hiv-treatment.html. Accessed November 28, 2022.
- 28 | National Institutes of Health Office of AIDS Research. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. December 18, 2019. Available at: https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult-and-adolescent-arv/initiation-antiretroviral-therapy. Accessed November 28, 2022.
- 29 | Kaiser Family Foundation. HIV Viral Suppression Rate in U.S. Lowest Among Comparable High-Income Countries, 2020 or Latest Year. June 3, 2022. Available at: https://www.kff.org/hivaids/slide/hiv-viral-suppression-rate-in-u-s-lowest-among-comparable-high-income-countries-2020-or-latest-year/. Accessed November 28, 2022.
- 30 | Carlisle M. ‘We just lost two years.’ How COVID-19 disrupted the fight against HIV. Time. October 6, 2022. Available at: https://time.com/6220020/covid-19-hiv-testing-treatment/.
- 31 | Shaw ML. What Is the true cost of the high price of ART? American Journal of Managed Care. February 3, 2020. Available at: https://www.ajmc.com/view/what-is-the-true-cost-of-the-high-price-of-art. Accessed November 29, 2022.
- 32 | McCann NC, Horn TH, Hyle EP, Walensky RP. HIV antiretroviral therapy costs in the United States, 2012-2018. JAMA Internal Medicine. 2020;180(4):601.
- 33 | AIDS Education & Training Center Program. Barriers to Viral Load Suppression Infographic. January 28, 2015. Available at: https://aidsetc.org/resource/barriers-viral-load-suppression-infographic. Accessed November 29, 2022.
- 34 | Ahmed A, Dujaili JA, Jabeen M, et al. Barriers and enablers for adherence to antiretroviral therapy among people living with HIV/AIDS in the era of COVID-19: A qualitative study from Pakistan. Front Pharmacol. 2021;12:807446.
- 35 | National Institute of Allergy and Infectious Disease. Antiretroviral Drug Discovery and Development. November 26, 2018. Available at: https://www.niaid.nih.gov/diseases-conditions/antiretroviral-drug-development. Accessed November 30, 2022.
- 36 | National Institutes of Heallth. NIH launches clinical trial of three mRNA HIV vaccines. March 14, 2022. Available at: https://www.nih.gov/news-events/news-releases/nih-launches-clinical-trial-three-mrna-hiv-vaccines. Accessed November 30, 2022.
- 37 | Silverman E. AIDS groups criticize Express Scripts for excluding several HIV medicines. STAT. June 6, 2019. Available at: https://www.statnews.com/pharmalot/2019/06/06/aids-hiv-express-scripts-formularies/. Accessed November 30, 2022.
- 38 | Evernorth.2021 Drug Trend Report 2021 and Onward. Available at: https://www.evernorth.com/drug-trend-report/2021-and-onward. Accessed November 30, 2022.
- 39 | Citroner G. Cost of HIV prevention drug discouraging people from doing PrEP therapy. Healthline. April 24, 2020. Available at: https://www.healthline.com/health-news/cost-of-hiv-prevention-drug-discouraging-people-from-doing-prep-therapy. Accessed November 30, 2022.
- 40 | Killelea A, Horn T. At last, generic HIV prevention drugs promise savings and access—but also reveal precarious financing. May 20, 2021. Health Affairs Forefront. Available at: https://www.healthaffairs.org/do/10.1377/forefront.20210519.54233. Accessed November 30, 2022.
- 41 | Whitfield T JS, Wachman M, Grov C, Parsons J, Rendina H. PrEP may offer psychological benefits to gay, bisexual men at risk for HIV. J Sex Res. 2019.
- 42 | World Health Organization.Global State of PrEP. Available at: https://www.who.int/groups/global-prep-network/global-state-of-prep. Accessed November 30, 2022.
- 43 | Kavanagh MM, Agbla SC, Joy M, et al. Law, criminalisation and HIV in the world: Have countries that criminalise achieved more or less successful pandemic response? BMJ Global Health. 2021;6(8):e006315.
- 44 | The Commonwealth Fund. The Latest Legal Challenge to the Affordable Care Act’s Preventive Services Guarantee. July 25, 2022. Available at: https://www.commonwealthfund.org/publications/explainer/2022/jul/latest-legal-challenge-affordable-care-act-preventive-services. Accessed November 30, 2022.
- 45 | Keith K. Court holds that key ACA preventive services requirements are unconstitutional. Health Affairs Forefront. September 8, 2022. Available at: https://www.healthaffairs.org/content/forefront/court-holds-key-aca-preventive-services-requirements-unconstitutional. Accessed November 30, 2022.
- 46 | World Health Organization. Why the HIV epidemic is not over. Available at: https://www.who.int/news-room/spotlight/why-the-hiv-epidemic-is-not-over. Accessed November 30, 2022.
More Topics
Articles & Guides
This content is for members only. Already a member?
Login
![]()